Report Summary
This study evaluates outcomes from April 2011 to May 2013 for 163 hospital patients screened by the 10th Decile Project in Los Angeles, which works with hospitals to identify the 10 percent of homeless patients with the highest public and hospital costs – the 10th decile – and provide immediate services for placing these individuals into permanent supportive housing. This is affordable housing that provides access to health and social services, such as mental health and addiction therapy, medical care, and case management. The triage tools that are used for screening employ accurate, simple to use statistical models that analyze information about individuals that is available in hospitals, jails and homeless service agencies affiliated with medical clinics to identify the one-tenth of homeless persons with the highest public costs and the acute ongoing crises that create those high costs. Because there are multiple paths into this highest-cost group, ranging from young persons with psychoses who are publicly disruptive to older persons are simply very sick, each tool uses a cluster of statistical models specifically designed to assess risk factors for different age and gender groups. An analysis of cost outcomes shows that housing 10th decile patients resulted in avoidance of significant public and hospital costs.
- For the 10th decile patients studied in this evaluation who obtained housing, total annual average public and hospital costs per person are estimated to have decreased from $63,808 when homeless to $16,913 when housed – excluding housing subsidy costs.
- Total health care costs, including jail medical and mental health care, are estimated to have declined an average of 72 percent, from $58,962 to $16,474 per person.
Taking costs for housing subsidies and supportive services into account, every $1 dollar in local funds spent to house and support 10th decile patients is estimated to reduce public and hospital costs for the evaluation population that was housed by $2 in the first year and $6 in subsequent years.  After taking account of the costs for helping these patients make the transition from homelessness to permanent supportive housing, subsidizing rent, and providing services to help them stay housed, the bottom line financial results from the evaluation are shown in the table. These cost avoidances are contingent on retaining 10th decile clients in permanent supportive housing, which is facilitated by higher rather than lower levels of on-site services, particularly given the severe problems of this population. Eighty percent of the patients screened were in the 10th decile. Patients typically had two or more physical disorders and 42 percent were triply diagnosed with physical, mental and substance abuse disorders.
After taking account of the costs for helping these patients make the transition from homelessness to permanent supportive housing, subsidizing rent, and providing services to help them stay housed, the bottom line financial results from the evaluation are shown in the table. These cost avoidances are contingent on retaining 10th decile clients in permanent supportive housing, which is facilitated by higher rather than lower levels of on-site services, particularly given the severe problems of this population. Eighty percent of the patients screened were in the 10th decile. Patients typically had two or more physical disorders and 42 percent were triply diagnosed with physical, mental and substance abuse disorders.
| Category | Amount | Description |
| Cost Avoidance (Gross) | $46,895 | Annual public costs avoided as a result of housing 10th decile patients for the evaluation population that was placed in permanent supportive housing ($63,808 in annual costs when homeless vs. $16,913 when housed) |
| 10th Decile Program Costs | $15,159 | One-time costs to house each patient, including the first year of local subsidies for rent and supportive services |
| $3,518 | Annual rent subsidy in the second and subsequent years, in addition to the Section 8 subsidy | |
| $3,000 | Annual cost for enriched supportive services in the second and subsequent years | |
| Cost Avoidance (Net) | $31,736 | Public costs avoided in the first year after paying the housing subsidy shortfall and one-time costs for housing placement, representing $2 in public costs avoided for every $1 spent in the first year |
| $40,377 | Public costs avoided, after paying for local housing subsidies and enriched supportive services, in the second year and each year that follows, as long as the patient remains housed. This represents $6 in public costs avoided for $1 spent for housing subsidies and supportive services |
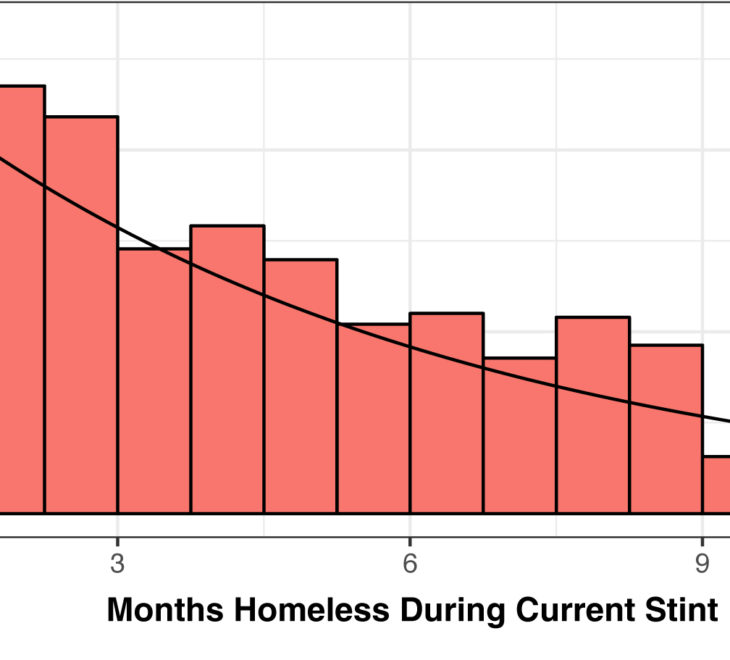
Sixty-eight percent of patients in the 10th decile were engaged as program participants by the navigators. This opened the door to immediate, comprehensive services and a path to permanent supportive housing. Virtually every patient who remained engaged obtained permanent supportive housing (98 percent), although this typically took six months and sometimes as long as two years.  This highly effective program can be strengthened and the proportion of high-cost, high-need homeless hospital patients whose needs are addressed through housing rather than through emergency hospital care can be increased through the following steps.
This highly effective program can be strengthened and the proportion of high-cost, high-need homeless hospital patients whose needs are addressed through housing rather than through emergency hospital care can be increased through the following steps.
Increase the Housing Supply
The most difficult problem facing the 10th Decile Project is lack of access to permanent supportive housing and extended delays in obtaining housing subsidy vouchers that enable patients to pay rent. This drives up the attrition rate. Broad housing solutions are needed to increase the supply of permanent housing and reduce time waiting to get into that housing. The following actions are recommended:
- Make more existing project-based permanent supportive housing units available to 10th decile renters.
- Convert tenant-based Section 8 vouchers into project-based vouchers that will provide the financial backbone for converting existing rental complexes into project-based permanent supportive housing sites.
- Make 10th decile individuals a top priority for tenant-based housing subsidies.
- Provide inclusive housing for 10th decile patients with a criminal background or immigration status that is a barrier to obtaining housing.
- Create an ongoing funding source such as housing impact fees for new development or real estate transfer fees to provide substantial, reliable funding for increasing the supply of affordable housing.
Increasing the Engagement Rate
Seventy-one percent of 10th decile patients were engaged by navigators or placed in another program. More of the remaining 29 percent of patients can be engaged by:
- Increasing the effectiveness of hospitals and navigators in achieving a warm hand-off of 10th decile patients.
- Flagging the hospital records of patients who decline to participate and encouraging them to reconsider this decision when they return to the hospital.
- Providing recuperative care or skilled nursing for patients who have health barriers that prevent them from living in permanent supportive housing.
- Improving the capacity of navigators to fill in behind each other in picking up referrals.
Increasing the Housing Rate
The long wait for permanent housing causes significant attrition. Attrition can be reduced and the housing rate increased by increasing funding for temporary housing with private rooms rather than dormitory-style emergency shelters, and notifying hospitals about the identities of missing clients so that they can be reconnected with their navigator when they return.
System Improvements
Hospitals are the primary financial beneficiaries when 10th decile patients are housed. Providing permanent housing with supportive services to several thousand 10th decile patients will make a striking reduction in the number of chronically homeless patients seen in hospitals, with tangible savings in hospital costs. Navigators and hospitals should jointly assess the savings that accrue to hospitals when 10th decile patients are placed in permanent supportive housing with ongoing services and identify a feasible and equitable level financial reciprocity for hospitals Hospitals should collaborate with the 10th Decile Project to screen all homeless patients in their databases in order to address systematically the problem of homeless patients who are frequent users of emergency health care services as well as to achieve system-wide cost reductions by housing these patients. In addition, hospitals in proximity to each other should integrate data for homeless patients and screen these integrated records to identify 10th decile individuals.
Next Steps
The next phase of the 10th Decile Project will address the recommendations in this evaluation including increasing the availability of permanent housing, expanding the base of financial support, and bringing the project to scale.
Research Citations and Press Coverage
Permanent Supportive Housing With Housing First: Findings From a Community Guide Systematic Economic Review
By Verughese, Jacob et al. American Journal of Preventive Medicine, Volume 61, Issue 5. (November 10, 2021)